Food Sci. Technol, Campinas, v42, e94321, 2022 1
Food Science and Technology
ISSN 0101-2061 (Print)
ISSN 1678-457X (Online)
OI: D https://doi.org/10.1590/fst.94321
1 Introduction
Foodborne diseases (FBDs) are a major public health issue
worldwide, especially for young persons, older persons, and those
who are sick (Fungetal., 2018). e World Health Organization
(WHO) denes FBDs as ‘diseases causing the infection or
poisoning of human bodies, usually caused by pathogens that
enter bodies through ingestion (Guoetal., 2018). In China, the
most common pathogens of foodborne diseases are Dysentery
bacilli, Typhoid bacilli, Salmonella, Vibrio parahaemolyticus
and Escherichia coli. e peak incidence of those pathogens
mentioned above is concentrated from July to September. And the
peak incidence of norovirus was concentrated from November
to May of the following year (Fuetal., 2019;Wuetal., 2021).
Microbial contamination is an important cause of morbidity
and mortality.
According to a report by the WHO, in 2010, 600 million people
fell ill globally, and 420,000 people died from FBDs. e global
burden FBDs caused in 2010 was 33 million disability adjusted
life years(DALYs) (Havelaaretal., 2015). Internationally, one
of the most notorious incidents is the Minamata disease caused
by methylmercury poisoning, which, released from factories,
accumulated in sh and shellsh and entered the body through
consumption, rst discovered in 1956 in Kumamoto Prefecture,
Japan (Fungetal., 2018). Another incident occurred in the Jinzu
river basin, Japan. e local residents along the river suered
an illness called ‘itai-itai’. e river and crops were polluted by
the sewage discharged from mining. us, cadmium entered
the body through water and rice consumption. is caused
a series of symptoms, with ostealgia as the main symptom
(Fungetal., 2018).
On average, one in every 6.5 people in China suers from
FBDs due to eating unsafe food (Chen, 2016). Food safety issues
are also causing concern. In 1988, an outbreak of hepatitis A
occurred in Shanghai due to consumption of raw clams, which
resulted in nearly 300,000 people suering from illness, and
11 deaths (Liuetal., 2018). In 2008, consumption of melamine-
tainted milk had sickened more than 294,000 infants and young
children, of whom 51,900 were hospitalised and resulted in at
least six deaths, mainly due to kidney problems (El-Nezamietal.,
2013). In 2011, in Henan province in China, many farms fed pigs
with fodder mixed with clenbuterol for economic benets. Once
an anti-asthma drug, clenbuterol is banned in fodder because
it brings great harm to humans through the consumption of
pork (Huetal., 2019).
Unsafe food not only aects human health and security, but
also threatens economic growth and social stability.Food safety
was ranked rst in the top ve safety issues in China (Lametal.,
Surveillance for foodborne diseases in a sentinel hospital in Jinhua city, Midwest of
Zhejiang province, China from 2016–2019
Fang-Rong XU
1
, Yang YANG
2
*
a
Received 19 Sep., 2021
Accepted 20 Oct., 2021
1
Department of Clinical Nutrition, Aliated Jinhua Hospital, Zhejiang University School of Medicine, Jinhua, Zhejiang, China
2
Department of Prevention and Health Care, Aliated Jinhua Hospital, Zhejiang University School of Medicine, Jinhua, Zhejiang, China
*Corresponding author: yangyangyy[email protected]
Abstract
To analysis the main clinical symptoms and causative hazards of foodborne disease outbreaks to provide a reference for the
prevention, control, and early warning of foodborne diseases. 2,919 FBDs cases were collected and summarised through the
China Food and Drug Administration (CFDA) surveillance system. Foodborne diseases were detected according to national
standards. Microso Excel 2010 and SPSS 12.0 were used for data descriptive analysis. e mean±standard deviation was used
to describe the numerical variables, and the frequency and composition ratio were used to describe the classication variables.
ere were 2,919 FBDs cases included in the analysis. e highest number of cases occurred among students (41.49%) and
farmers (22.85%). e months of August (398,13.63%), September (333,11.41%) and July (330,11.31%) accounted for most cases.
e two most frequent pathogens supported by laboratory conrmation are Norovirus and Salmonella. e major symptoms
of illness were diarrhoea (97.64%), fever (27.95%), abdominal pain (24.67%), vomiting (22.30%), and nausea (13.7%). is
study revealed epidemiological characteristics of FBDs and identied some higher risk factors for interventions. Salmonella
and Norovirus were the main pathogens. Foods from catering service settings and animal foods were the factors most likely to
contribute to foodborne diseases. Most cases of intoxication and outbreaks were related to wild mushrooms.
Keywords: foodborne diseases; surveillance; epidemiology; risk factors.
Practical Application: is article provided clues for health education of community oriented, school oriented or other society
groups.
Original Article
Food Sci. Technol, Campinas, v42, e94321, 20222
Surveillance for foodborne diseases
2013). In 2009, the China Food and Drug Administration (CFDA)
set up the FBDs surveillance system to ensure food safety and
prevent unnecessary foodborne illnesses. is included checking
for pathogenic microorganisms, food products and plants entering
the food supply, and chemical contamination (Wuetal., 2018).
e system monitored FBDs cases, outbreaks and suspected risk
factors to identify potential hazards. Zhejiang Province started the
FBDs surveillance system in 2010. To date, 31 major surveillance
hospitals are involved. e Aliated Jinhua Hospital, Zhejiang
University School of Medicine, as the biggest sentinel hospital
in midwest Zhejiang, is among them.
Previous literature shows there were few studies from the
perspective of hospitals. e objective of this study is to describe
the demographic and epidemiological characteristics of FBDs
surveillance carried out by Aliated Jinhua Hospital, Zhejiang
University School of Medicine during 2016–2019. Furthermore,
it provided several recommendations for policy perfection and
cooperation between hospitals and centres for disease control
and prevention (CDC).
2 Materials and methods
2.1 Case denition
FBDs cases are dened as patients with diarrhoea (frequency
equal or greater than three instances of abnormal stool characters)
or vomiting or toxic symptoms suspected of being caused by food
consumption. An outbreak is dened as two or more patients
with FBDs who consumed the same food prior to the onset of
illness at a similar time, and the clinical manifestations of all
poisoned patients are basically similar.
2.2 Data sources
We collected and summarised data through the CFDA’s
surveillance system. 2,919 FBDs cases were selected in a sentinel
hospital in Jinhua city from 2016–2019, and 1,651 (56.56%) were
male, while 1,268 (43.44%) were female. e information was
collected for the number of outpatients and patients hospitalised
due to diarrhoea. Each patient’s details included gender, age,
occupation, home address, contact information, diet, duration
of disease, clinical symptoms of illness, suspected food vehicle,
setting of food preparation or consumption and the number of
cases by suspected causative hazards. Stool samples (only from
patients with diarrhoea) were collected and sent to the laboratory
for conrmation, and they are mainly detected by bacterial
culture and molecular biology. All the laboratory examination
methods were executed in accordance with national standards
(GB47894-2010, GB47895-2003, GB47897-2008 and GB47896-
2003) and the testing procedures specied in e Manual of
2014 National Foodborne Disease Monitoring Work.
2.3 Food vehicle classication
Food vehicles were combined into nine classications for
clarity. For example, meat products and aquatic animal products
were included in animal foods. Vegetable products, fruit products
and fungi products were included in plant foods. Multiple foods
refer to consuming two or more classications of foods. Blended
foods refer to a mixture of two or more classications of foods,
such as dumplings.
2.4 Data analysis
2,919 FBDs cases were derived from the CFDA surveillance
system. SPSS12.0 were used to carry out descriptive analysis of
numerical variables, frequency and composition ratio analysis
of categorical variables.
3 Results
3.1 Demographic distribution
Of 2,919 FBDs cases from 2016–2019, 2,480 cases reported
suspected food. e 0~, 16~ and 26~ age group had higher
percentages. Students and farmers are high risk groups of food
poisoning, accounting for 41.49% and 22.85% of the total cases,
respectively. (Table1).
3.2 Time distribution
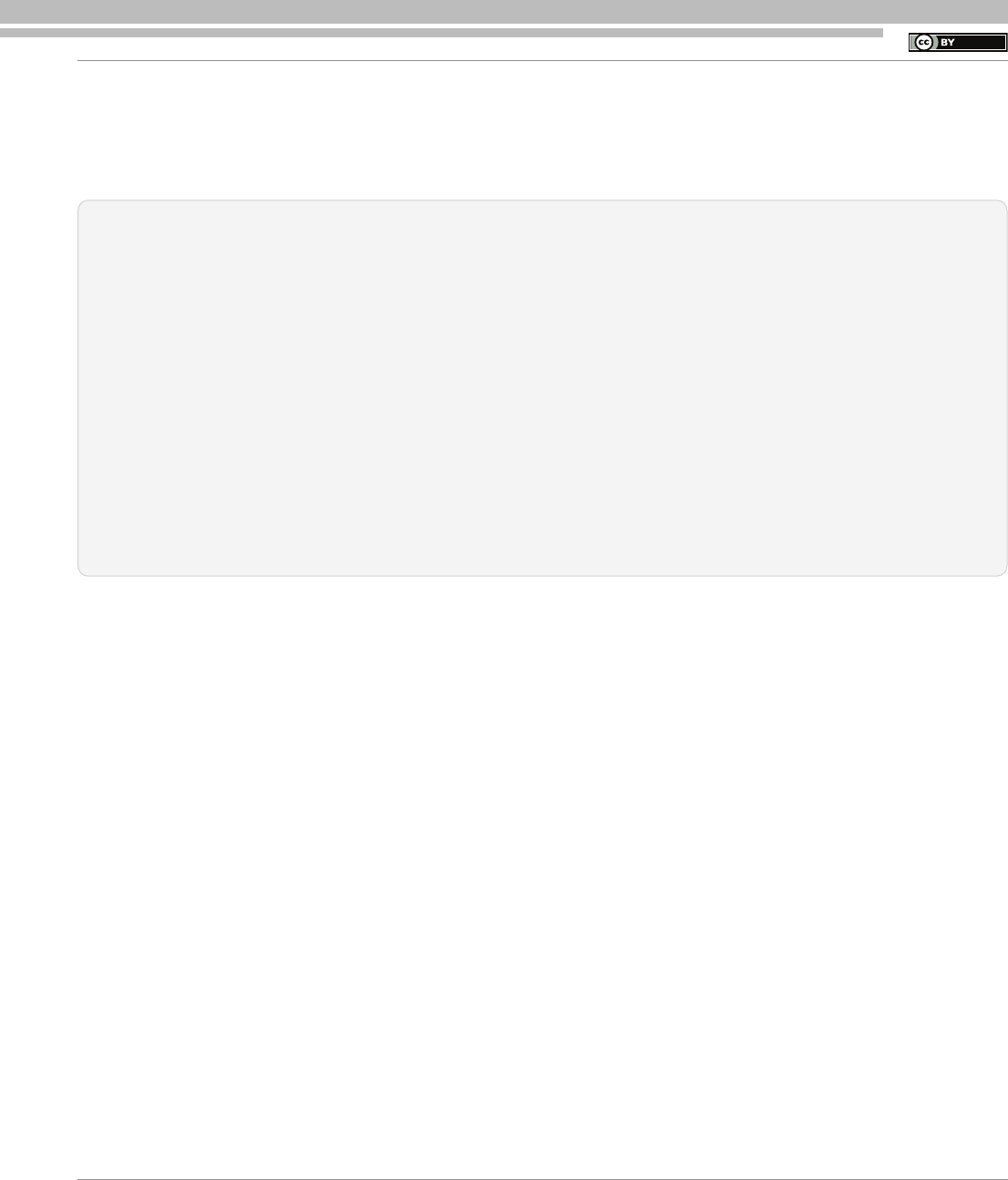
e months of August (398, 13.63%), September (333, 11.41%)
and July (330, 11.31%) accounted for most cases. e fewest
cases occurred in the January to April period (Figure1). e two
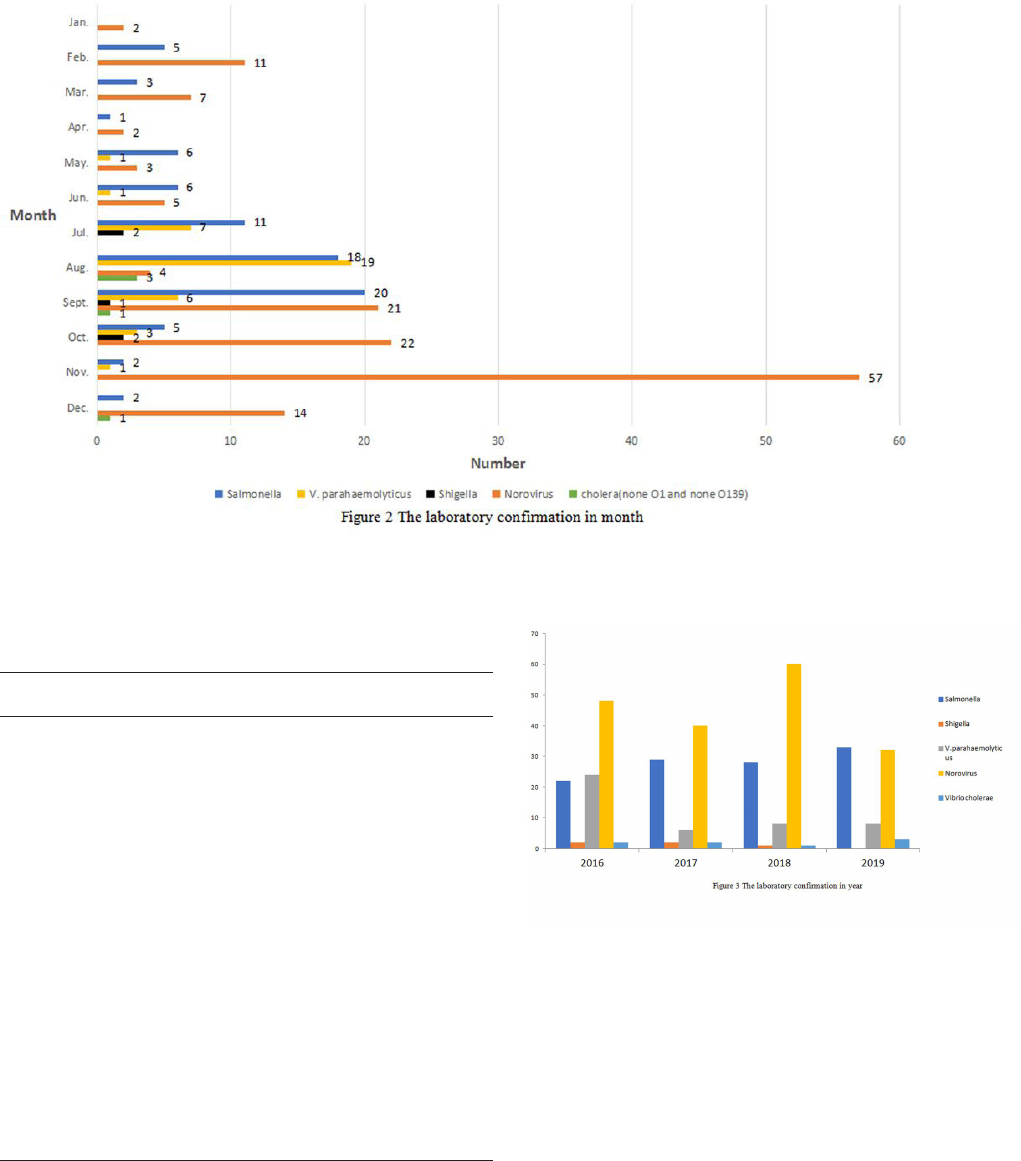
most frequent pathogens supported by laboratory conrmation
are Norovirus and Salmonella (Figure2and3).
3.3 Number of patients and hospital admissions due to
diarrhoea
From 2016–2019, the number of outpatients suering
from diarrhoea made up an average of 0.67% (0.53%–0.87%)
of the total patients. e number of patients hospitalised due to
diarrhoea made up an average of 0.53% (0.38%–0.74%) of the
total hospitalised patients.
3.4 Main clinical symptoms of illness
e major symptoms of illness were diarrhoea (97.64%),
fever (27.95%), abdominal pain (24.67%), vomiting (22.30%),
and nausea (13.7%). e clinical symptoms of cases are shown
in detail in Table 2 and Figure 4.
3.5 Setting of food preparation or consumption, and
suspected food vehicles
Of 2,919 FBDs cases, 2,480 patients were willing or able to
provide information about food consumption in terms of food
processing and packaging methods. Catering services accounted
for 979 cases (39.48%). Homemade food was the second most
common method, accounting for 840 cases (33.87%), followed
by bulk food (273 cases, 11.01%), other methods (229 cases,
9.23%) and prepackaging (159 cases, 6.41%). Nine food
classications were detected. e top ve were animal foods
(798 cases, 32.18%), multiple foods (405 cases, 16.33%), plant
foods (369 cases, 14.88%), milk and beans (263 cases, 10.60%)
and others, mainly including lactation of human milk (303 cases,
12.22%) (Table3).
Original Article
Xu; Yang
Food Sci. Technol, Campinas, v42, e94321, 2022 3
3.6 Causative hazards
e causative hazards were classied into infectious and
cases of intoxication. With decreased immunity, the human body
produces less antibody synthesis. is enhances the number of
infectious cases. Poisoning cases occurred due to misuse of toxic
wild mushrooms and herbs or misuse of pesticides. Consuming
wild mushrooms resulted in the majority of cases of intoxication
and outbreaks (Table4).
4 Discussion
From 2001 to 2010, 5,021 outbreaks of FBDs were reported
in China, causing 140,101 illnesses and 1,427 deaths (Lietal.,
2018). FBDs cause a huge burden of disease globally, especially
in less developed countries. As a typical developing country,
China’s economy has developed rapidly since the reform and
opening period. However, public health systems like food safety
surveillance in China did not improve until the outbreak of
SARS in 2002, which posed serious challenges. e food safety
incidents mentioned above have not only heavily damaged
China’s food industry and exports but also done serious harm
to its national reputation and international image. Worryingly,
the more serious accompanying negative eects have not been
completely eliminated.
Table 1. Demographic distribution of foodborne disease cases.
Classication Number of cases Percent(%) Classication Number of cases Percent(%)
Gender Year
Male 1651 56.56 2016 923 31.62
Female 1268 43.44 2017 732 25.08
Age group(yr.) 2018 677 23.19
0~ 732 25.08 2019 587 20.11
6~ 260 8.91
16~ 367 12.57
26~ 367 12.57
36~ 253 8.67
46~ 304 10.41
56~ 309 10.59
66~ 327 11.20
Occupation
Students(include
preschoolers)
1211 41.49
Farmers 667 22.85
Oce sta 310 10.62
Workers 283 9.70
Commercial service 275 9.42
Unemployed 146 5.00
Catering services 10 0.34
Other 17 0.58
Tot a l 2919 100 Tot a l 2919 100
Figure 1. Number of cases in month.
Table 2. Clinical symptoms of foodborne disease cases.
Main clinical
symptoms
Number of cases Rate(%)
Diarrhea 2850 97.64
Fever 816 27.95
Abdominal pain 720 24.67
Vomiting 651 22.3
Nausea 400 13.7
Hypourocrinia 138 4.73
irst 61 2.09
Dehydration 49 1.68
Wea k ness 36 1.23
Tic 30 1.03
Chills 29 0.99
Convulsions 15 0.51
Original Article
Food Sci. Technol, Campinas, v42, e94321, 20224
Surveillance for foodborne diseases
In our study, the patients’ symptoms are mainly diarrhoea,
fever, abdominal pain, vomiting and nausea, as shown in other
studies. Infectious cases usually have digestive symptoms of
diarrhoea, abdominal pain or vomiting. As the leading symptom
of FBDs, diarrhoeal disease is also one of the leading causes
of death in children under ve (Asefaetal., 2020). In a single
hospital like ours, within four years, 53,733 (0.67%) outpatients
seek treatment due to diarrhoea. Among these patients,
2,658 (0.57%) were hospitalised (Table2). is causes great
health and nancial burden to patients, as well as increasing
doctors’ workloads. Further, the risk of hospital infection could
be a threat to other patients.
Males were more likely to suer from FBDs, as men were
generally more adventurous than women when making irrational
decisions (Shanetal., 2019). Children under six were more likely
to suer FBDs, as mentioned in the previous study (Havelaaretal.,
2015), due to their lower immunity and the absence of health
education. Preschoolers and students accounted for more than
60% of cases. is is partly due to their lower immunity, as
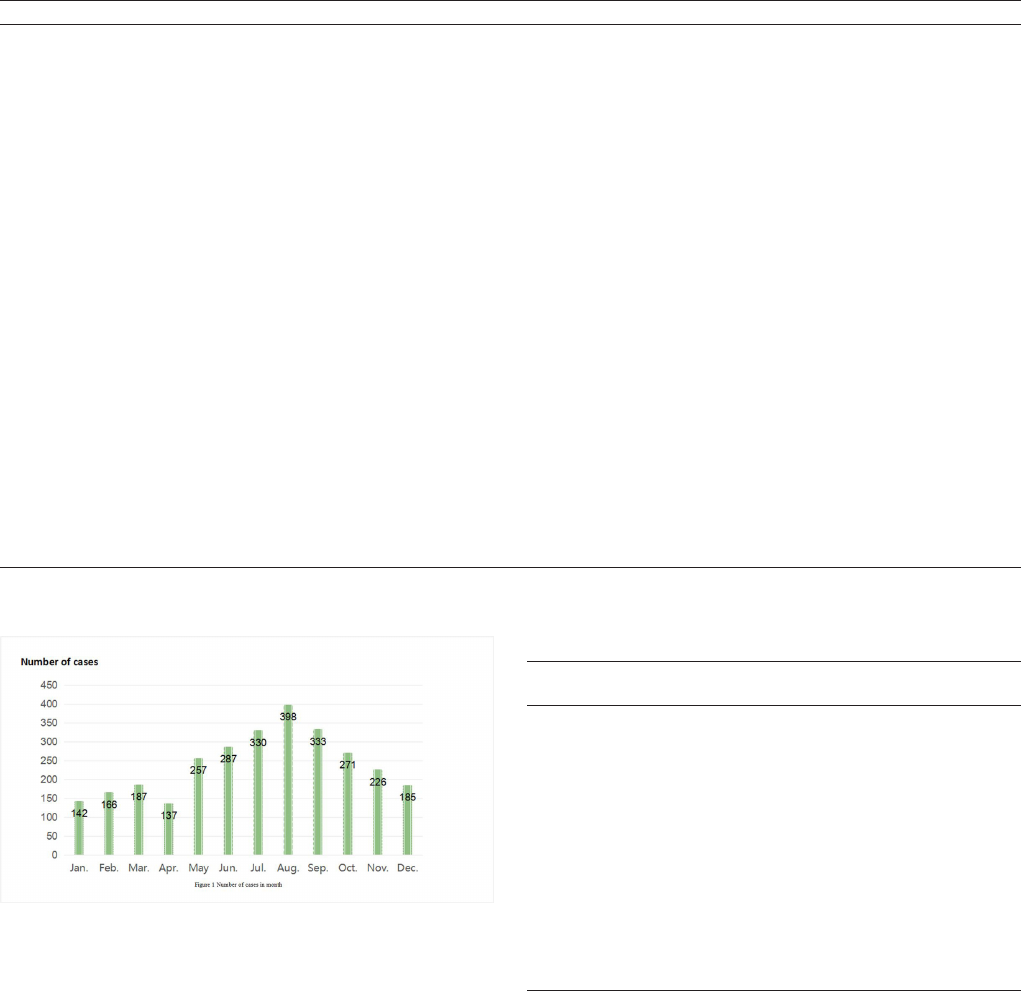
Figure 2. e laboratory comrmation in month.
Figure 3. e laboratory comrmation in year.
Table 3. Number and proportion of food preparation or consumption
and vehicle.
Number of
cases
Percent(%)
Setting of food preparation or
consumption
Catering services 979 39.48
Homemade 840 33.87
Bulk food 273 11.01
Prepackaging 159 6.41
Else ( lactation of human milk, etc) 229 9.23
Suspected food vehicle
Animal foods 798 32.18
Multiple foods 405 16.33
Plant foods 369 14.88
Milk and bean 263 10.6
Blended foods 143 5.77
Cereals 95 3.83
Drinks 75 3.02
infant foods 29 1.17
Else(Sweetmeat, Nut, condiment, Algae,
etc)
303 12.22
Tot a l 2480 100
Original Article

Xu; Yang
Food Sci. Technol, Campinas, v42, e94321, 2022 5
mentioned above. is is also due to their lack of control over
their diets and the likelihood that they consume food at roadside
stands which usually have poor sanitary conditions. Signicantly,
farmers made up a h of all cases. Compared with developed
countries, most farmers in China belong to a low-income group.
erefore, they pay little attention to the food safety and hygiene
and consumption settings and, thus, are more likely to be invaded
by pathogens through contaminated food.
e seasonality of FBDs cases was observed in this study.
Most cases occurred in warm months (May to October), peaking
in summer. is was in line with other studies (Wu etal.,
2021;Lietal., 2018). On the one hand, high temperatures are
conducive to pathogen growth, as is known (Yangetal., 2019).
On the other hand, insects such as ies multiply rapidly when
the temperature is appropriate, and pathogens spread to many
places, along with those hosts’ movements. As showed in Figure2,
bacteria like Salmonella, V. parahaemolyticus, Shigella and
cholera (none O1 and none O139) were commonly detected
in warm months. However, a seasonal peak in summer does
not occur for some pathogens. For instance, Norovirus is more
frequent in winter months when the temperature is relatively
low (Halletal., 2012). Certainly, temperatures are not the only
factors with seasonality. Humidity, light or other climatic factors
could also inuence pathogen growth (Parketal., 2018).
Causative hazards will invade food during each link of
preservation and processing, such as food storage, food preparation,
cooking, the cooking environment, the hand hygiene of cooks
and pantry helpers and tableware disinfecting (Yangetal.,
2019;Brownetal., 2017). One well-known person was ‘Typhoid
Mary’ who brought typhoid to places where she worked as a
cook (Fegan & Jenson, 2018). About 40% of patients with FBDs
reported consuming food from catering service settings prior to
the onset of illness. In recent years, it has become fashionable
to order takeaway food through apps. is brings more unsafe
factors since it is dicult to supervise the quality of food and the
preparation process for those without xed shops. In addition,
due to the complexity of Chinese food and cooking methods,
pathogens could contaminate foods in more ways, making it
dicult to avoid FBDs. e main food vehicles suspected of
causing illnesses are animal foods and multiple foods. As it is
known, animal foods can provide hotbeds for pathogens if not
stored properly and, thus, cause diseases (Marr, 1999). Similar
to other studies (Wuetal., 2019;Fingeretal., 2019), multiple
foods remain one of the most common vehicles, and this presents
diculties in identifying the specic foods and preventing them
from circulation. It should be noted that homemade foods led
to more than 30% of cases. As shown above, 1.48% of FBDs
cases and 20% of the FBDs outbreaks related to people picking
wild mushrooms, herb or agaric and consuming them at home,
even consuming pesticide by mistake. All of this suggested the
absence of food safety education for the general public.
With globalisation, the problems of food safety will not
be restricted to a single country or region. In China, a large
population, environmental pollution, regional development
imbalances and public health system construction remain
crucial. Challenges are upon us, not merely to hospitals but also
government agencies, CDC, health supervision agencies and
food enterprises. Government agencies must reinforce laws to
strengthen food safety. Hospitals should be on the alert for FBDs
cases, provide proper treatment and share information with CDC
as well as other health supervision agencies or organisations.
As the source of the food supply chain, food enterprises must
stick to the rules and regulation on food safety and hygiene to
make people safe.
Some limitations exist in this study. First, we did not use any
sequencing or genomic methodologies. e use of the power
of whole genome sequencing in combination with laboratory
methods in order to understand genetic dierences between
pathogens and to conduct surveillance of diseases. Second, a few
patients failed to provide information about food consumption.
It reduced the available data of food consumption characters
to a degree. ird, when considering dierent diagnostic levels
and a lack of laboratory conrmation, a small number of cases
that might not be classied as FBDs were included in the study.
ese cases may provide some interference information for
analysis. Fourthly, this study was conducted in only one hospital.
In the future, we hope more hospitals in Jinhua city will join the
surveillance system. e data from each hospital will be combined
and be more representative of the whole city. Finally, only a few
pathogens were identied by the laboratory for conrmation,
resulting in some pathogens not being detected. We hope that in
future, more pathogens will be included and that this will improve
the rate of laboratory conrmation. us, suggestions from
studies will be more targeted for policymakers and supervisors.
In these future studies, we will make improvements according
to the above limitations.
Table 4. Number of cases by suspected causative hazards.
Causative hazards Number of cases Percent(%)
Infectious cases 2876 98.52
Toxic cases 43 1.48
Wild mushrooms 28 0.96
Herb 11 0.38
Agaric 2 0.07
Pesticide 2 0.07
Figure 4. Pathogen constituents.
Original Article
Food Sci. Technol, Campinas, v42, e94321, 20226
Surveillance for foodborne diseases
Fegan, N., & Jenson, I. (2018). The role of meat in foodborne disease: Is
there a coming revolution in risk assessment and management? Meat
Science, 144, 22-29. http://dx.doi.org/10.1016/j.meatsci.2018.04.018.
PMid:29716760.
Finger, J. A. F. F., Baroni, W. S. G. V., Maffei, D. F., Bastos, D. H. M., &
Pinto, U. M. (2019). Overview of foodborne disease outbreaks in
Brazil from 2000 to 2018. Foods, 8(10), 434. http://dx.doi.org/10.3390/
foods8100434. PMid:31547589.
Fu, P., Wang, L. S., Chen, J., Bai, G. D., Xu, L. Z., & Guo, Y. C. (2019).
Analysis of foodborne disease outbreaks in China mainland in 2015.
Zhongguo Shipin Weisheng Zazhi, 31(01), 64-70.
Fung, F., Wang, H. S., & Menon, S. M. (2018). Food safety in the 21st
century. Biomedical Journal, 41(2), 88-95. http://dx.doi.org/10.1016/j.
bj.2018.03.003. PMid:29866604.
Guo, S., Lin, D., Wang, L. L., & Hu, H. (2018). Monitoring the results
of foodborne diseases in Sentinel Hospitals in Wenzhou city, China
from 2014 to 2015. Iranian Journal of Public Health, 47(5), 674-681.
PMid:29922609.
Hall, A. J., Eisenbart, V. G., Etingüe, A. L., Gould, L. H., Lopman, B.
A., & Parashar, U. D. (2012). Epidemiology of foodborne norovirus
outbreaks, United States, 2001-2008. Emerging Infectious Diseases,
18(10), 1566-1573. http://dx.doi.org/10.3201/eid1810.120833.
PMid:23017158.
Havelaar, A. H., Kirk, M. D., Torgerson, P. R., Gibb, H. J., Hald, T.,
Lake, R. J., Praet, N., Bellinger, D. C., Silva, N. R., Gargouri, N.,
Speybroeck, N., Cawthorne, A., Mathers, C., Stein, C., Angulo, F.
J., & Devleesschauwer, B. (2015). World Health Organization global
estimates and regional comparisons of the burden of foodborne
disease in 2010. PLoS Medicine, 12(12), e1001923. http://dx.doi.
org/10.1371/journal.pmed.1001923. PMid:26633896.
Hu, D. W., Liu, C. X., Zhao, H. B., Ren, D. X., Zheng, X. D., & Chen,
W. (2019). Systematic study of the quality and safety of chilled pork
from wet markets, supermarkets, and online markets in China.
Journal of Zhejiang University Science B., 20(1), 95-104. http://dx.doi.
org/10.1631/jzus.B1800273. PMid:30614233.
Lam, H. M., Remais, J., Fung, M. C., Xu, L. Q., & Sun, S. S. M. (2013).
Food supply and food safety issues in China. Lancet, 381(9882),
2044-2053. http://dx.doi.org/10.1016/S0140-6736(13)60776-X.
PMid:23746904.
Li, Y. Q., Huang, Y. L., Yang, J. J., Liu, Z. H., Li, Y. M., Yao, X. T., Wei, B.,
Tang, Z. Z., Chen, S. D., Liu, D. C., Hu, Z., Liu, J. J., Meng, Z. H., Nie,
S. F., & Yang, X. B. (2018). Bacteria and poisonous plants were the
primary causative hazards of foodborne disease outbreak: a seven-
year survey from Guangxi, South China. BMC Public Health, 18(1),
519. http://dx.doi.org/10.1186/s12889-018-5429-2. PMid:29669556.
Liu, J. K., Bai, L., Li, W. W., Han, H. H., Fu, P., Ma, X. C., Bi, Z. W., Yang,
X. R., Zhang, X. L., Zhen, S. Q., Deng, X. L., Liu, X. M., & Guo, Y.
C. (2018). Trends of foodborne diseases in China: lessons from
laboratory-based surveillance since 2011. Frontiers of Medicine, 12(1),
48-57. http://dx.doi.org/10.1007/s11684-017-0608-6. PMid:29282610.
Marr, J. S. (1999). Typhoid mary. Lancet, 353(9165), 1714. http://dx.doi.
org/10.1016/S0140-6736(05)77031-8. PMid:10335825.
Park, M. S., Park, K. H., & Bahk, G. J. (2018). Interrelationships
between Multiple Climatic Factors and Incidence of Foodborne
Diseases. International Journal of Environmental Research and Public
Health, 15(11), 2482. http://dx.doi.org/10.3390/ijerph15112482.
PMid:30405044.
Shan, L., Wang, S. S., Wu, L. H., & Tsai, F. S. (2019). Cognitive biases
of consumers’ risk perception of foodborne diseases in China:
examining anchoring effect. International Journal of Environmental
is study revealed epidemiological characteristics of
FBDs in our hospital and identied some higher risk factors for
interventions. is study revealed epidemiological characteristics
of FBDs and identied some higher risk factors for interventions.
Males and preschool children were more likely to suer FBDs.
Salmonella and Norovirus were the main pathogens. Foods from
catering services settings and animal foods were the factors that
most oen contribute to foodborne diseases. Most of the cases
of intoxication and outbreaks were related to wild mushrooms.
Some information was provided to the government and other
organisations for further policy-making and supervision to
ensure food safety.
Ethical approval
e study was conducted in accordance with the Declaration
of Helsinki and the protocol was approved by the Ethics
Committee of Aliated Jinhua Hospital, Zhejiang University
School of Medicine (2019-301).
Conict of interest
e authors declare that they have no competing interests.
Availability of data and material
All data generated or analyzed during this study are included
in this published article.
Funding
Not applicable.
Author contribuitions
ese authors contributed equally to this study.
Acknowledgements
No funding or sponsorship was received for this study or
publication of this article.
References
Asefa, A., Qanche, Q., Asaye, Z., & Abebe, L. (2020). Determinants
of delayed treatment-seeking for childhood diarrheal diseases in
Southwest Ethiopia: a case-control study. Pediatric Health, Medicine
and erapeutics, 11, 171-178. http://dx.doi.org/10.2147/PHMT.
S257804. PMid:32607050.
Brown, L. G., Hoover, E. R., Selman, C. A., Coleman, E. W., & Rogers,
H. S. (2017). Outbreak characteristics associated with identification
of contributing factors to foodborne illness outbreaks. Epidemiology
and Infection, 145(11), 2254-2262. http://dx.doi.org/10.1017/
S0950268817001406. PMid:28689510.
Chen, J. S. (2016). Who is the number one enemy of food safety?.
Dietetic Science, 2016(5), 20.
El-Nezami, H., Tam, P. K. H., Chan, Y., Lau, A. S. Y., Leung, F. C. C.,
Chen, S. F., Lan, L. C. L., & Wang, M. F. (2013). Impact of melamine-
tainted milk on foetal kidneys and disease development later in life.
Hong Kong Medical Journal, 19(Suppl 8), 34-38. PMid:24473527.
Original Article
Xu; Yang
Food Sci. Technol, Campinas, v42, e94321, 2022 7
Epidemiology of foodborne disease outbreaks from 2011 to 2016 in
Shandong Province, China. Medicine, 97(45), e13142. http://dx.doi.
org/10.1097/MD.0000000000013142. PMid:30407341.
Wu, X., & Xu, D., Ji, L., Zha, Y., & Chen, L. (2021). Surveillance results
of foodborne diseases in Huzhou, Zhejiang, 2018–2020. Disease
Surveillance, 36(9), 958-962.
Yang, L., Sun, Y. B., Zhong, Q., Duan, D. S., Liu, S. Q., & Zhang, Y.
(2019). Epidemiological characteristics and spatio-temporal patterns
of foodborne diseases in Jinan, Northern China. Biomedical and
Environmental Sciences, 32(4), 309-313. PMid:31217068.
Research and Public Health, 16(13), 2268. http://dx.doi.org/10.3390/
ijerph16132268. PMid:31252539.
Wu, G., Wang, L. S., Wang, Q., Han, R., Zhao, J. S., Chu, Z. H., Zhuang,
M. Q., Zhang, Y. X., Wang, K. B., Xiao, P. R., Liu, Y., & Du, Z. J. (2019).
Descriptive study of foodborne disease using case monitoring data
in Shandong province, China, 2016-2017. Iranian Journal of Public
Health, 48(4), 722-729. http://dx.doi.org/10.18502/ijph.v48i4.1006.
PMid:31110983.
Wu, G., Yuan, Q., Wang, L. S., Zhao, J. S., Chu, Z. H., Zhuang, M. Q.,
Zhang, Y. X., Wang, K. B., Xiao, P. R., Liu, Y., & Du, Z. J. (2018).
Original Article
