University of Rochester
University of Rochester Medical Center
Eastman Institute for Oral Health
625 Elmwood Avenue
Rochester, New York 14620-2989 USA
(585) 275-8315
LETTER OF RECOMMENDATION FORM
Send this form to the person who is writing on your behalf. A pre-stamped and pre-addressed envelope should be included with each of the Letter of
Recommendation form. The envelope should be addressed to the Residency Coordinator at the address noted above.
PART 1 ~ Applicant should complete this section:
I, _______________________________________________________________________________________________________am
FIRST MIDDLE LAST
applying to the ______________________________________________________________ at the Eastman Institute for Oral Health.
PROGRAM OF STUDY TITLE/NAME
I do ________ do not ________ agree to waive my right under The Family Education Rights and Privacy Act of 1974 to review
specific and composite letters of recommendation.
________________________________________________________________________________________________________________________
Name (printed) Signature Date
Name of individual writing recommendation: ___________________________________________________________________________________
Print Name
PART 2 ~ Individual writing the recommendation should complete this section:
The Admissions Committee would appreciate your individual comments of the applicant’s preparation, aptitude, initiative and creativity necessary
for independent work and the motivation or strength of commitment to the professional career implied by this program of study. If you have taught
the applicant, your comparison of the applicant to other students who have done postdoctoral work elsewhere would be valuable.
Please return your recommendation as soon as possible as the Committee considers these letters a vital part of the application process. Please feel
free to use separate sheet of paper if needed.
How long have your known the applicant? __________________
In what capacity? ___________________________________________________________________________________________________
How would you rate the applicant among the students at a similar level that you have known in recent years?
Upper 10% ________ Upper 25% ________ Upper 50% ________ Lower 50% ________
Letters of Recommendation – EIOH Educational Training Programs Page 1 of 2 Revised Mar 2014
__________________________________________________________________________________________________________________
APPLICANT’S FIRST NAME MIDDLE LAST NAME
Letters of Recommendation – EIOH Educational Training Programs Page 2 of 2 Revised Mar 2014
PART 2 (continued)
If known, please give this student’s average class standing _______________ out of _______________ (class size).
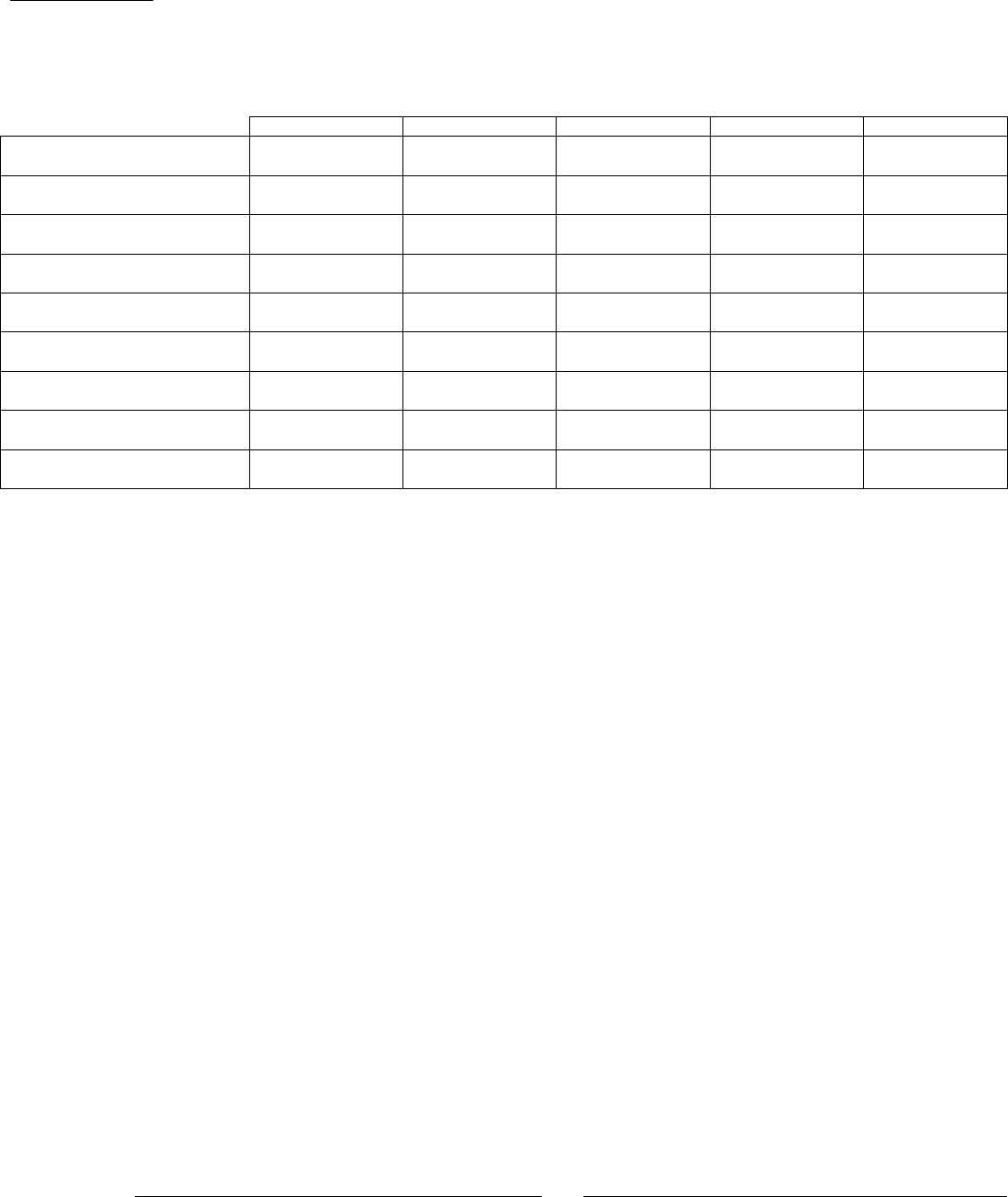
Please complete the following assessment of the applicant:
Excellent
Good
Average
Below Average
Unknown
Personality & Manners
Scientific Performance
Clinical Skills
Industry
Reliability
Initiative
Cooperation
Empathy & Compassion
Personal Hygiene & Neatness
Please provide your comments on the applicant’s personal demeanor and professional aptitude for the program.
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
This student is: ________ Recommended ________ Highly Recommended
________________________________________________________________________________________________________________________
Name (printed) Signature Date
Position, profession or occupation: ___________________________________________________________________________________________
Professional address: _____________________________________________________________________________________________________
Business/Company Name
________________________________________________________________________________________________________________________
Street City State Zip Country
Phone Numbers:
Work
Fax
